According to WHO statistics 39 million people in the world are blind. The leading cause for blindness in the world is cataract. Cataract, derived from the Greek word meaning a waterfall, is the clouding of the normally transparent lens in the eye. Changes that take place in the protein molecules in the lens is the cause for this.
It is common knowledge that age is the main cause of cataract. In addition, injuries to the eye, long term systemic illnesses such as diabetes mellitus, long term use of Steroid medications and smoking are also known to be associated with cataract.
The main symptom of cataract is the gradual onset of blurring of vision. As the cataract progresses, vision deteriorates further and the definitive treatment is surgery. Cataract surgery is the most common surgery performed in the world today, and has a high success rate with minimal discomfort to the patient. However, the evolution of cataract surgery is a long story.
History
The earliest records of Cataract surgery hails from India. According to reported history Cataract surgery was performed before 800 BC in Sushrutha’s Era where mature cataracts were pushed into the vitreous cavity using a sharp instrument, a technique known as couching.
In the western world, the French ophthalmologist Jacques Daviel (1696–1762) was the first modern European physician to successfully extract cataracts from the eye. However, as the lens was not replaced the patient had to depend on thick glasses to get useful vision.
Later on, the technique of surgery changed and the cataractous lens was removed leaving its capsule behind. This technique was named “extra capsular cataract extraction”.
In 1950, an English eye surgeon Sir Harold Ridley implanted the first artificial intra ocular lens made out of Poly Methyl Metha Acrylate (PMMA) successfully. This innovation was the result of Dr Ridley’s finding that the Second World War pilots who had this particular type of plastic accidentally implanted in the eye during warfare, showed no foreign body reaction during follow up.
Another breakthrough in the history of cataract surgery was the invention of the Phaco -emulsification machine. Fifty years ago in 1967, an American eye surgeon named Charles Kelman developed the Phaco machine after observing his colleague using ultra sound energy in dental surgery.
Intra ocular lens
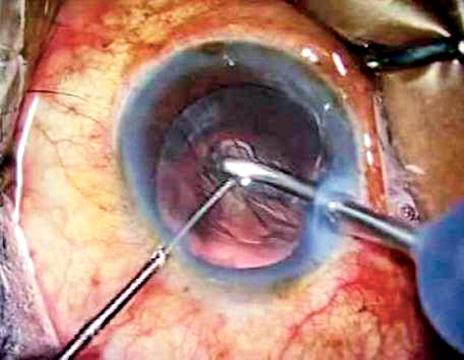
Nowadays, in many countries, including Sri Lanka the cataract surgery is carried out using the modern technology of ultra sound energy (Phaco -emulsification) and a foldable intra ocular lens is inserted through a 2.2 mm corneal incision causing minimal discomfort and speedy visual rehabilitation to the patient.
The future of cataract surgery involving laser energy is catching up and growing one’s own lens from stem cells as replacement is in the horizon with encouraging research outcomes.
However, the challenges those pioneering eye surgeons in Sri Lanka had to face to establish a state-of-the-art cataract surgery service in the country were also noteworthy. In the beginning, they had to pursue the necessary training on their own and even obtaining sophisticated micro-instruments had to be self funded. As the government could not provide phaco machines at a cost of more than 1.1 million rupees to each hospital at the beginning, other avenues had to be resorted to. The suppliers of intra ocular lenses agreed to provide the machines and patients in government hospitals also had the privilege of undergoing cataract surgery with the modern techniques.
More recently, the government decided to regulate the prices of the intra ocular lenses and also provide the lenses free of charge to patients undergoing surgery in the government sector. The eye surgeons pledged their fullest support to both decisions and on the request of the Health Ministry provided the specifications for good quality intra ocular lens to be purchased by the government. Ethically, clinicians need to ensure they are providing the best for their patients and have a sound rationale for the advice they provide in comprehensive terms of safety, and outcomes.
However, new problems arose as the suppliers of phaco machines now were reluctant to provide the same service facility at no cost as their profit margin was limited and the procurement of lenses by the government takes a longer duration due to procedural delays.
As of today, the country has a prevalence of blindness in 1.7% among the age 40+ population, with 67 % having cataract according to the blindness survey carried out in 2014/2015. The government, health professionals, NGOs and industry should work as a team and take necessary measures to achieve the goal towards eliminating avoidable blindness in the country.
The writer is Consultant Eye Surgeon /Senior Lecturer Faculty of Medicine,
University of Colombo