The recent pledge by the Government to end preventable stillbirths, a hitherto neglected area has been welcomed as a step in the right direction following concerns over the rise in the number of perinatal (fetal) deaths. Following this an effort to delve into the causes and analyse data on such deaths has also been taken. The Maternal and Child Morbidity and Mortality Surveillance Unit of the Family Health Bureau, is confident it can reach that goal through its ongoing systematic collection and dissemination of analysed data to relevant persons for action.
National Program Manager, Maternal & Child Health Surveillance, and Community Physician FHB, Ministry of Health, Dr Kapila Jayaratne tells the Sunday Observer why analysing and disseminating data on perinatal deaths is important for ensuring good pregnancy birth outcomes in future and reduce perinatal deaths in the country.
 Excerpts…
Excerpts…
Q. In recent years, perinatal mortality has become a focal point of attention to health officials the world over including Sri Lanka. Since many of our readers are not familiar with this term tell us what is perinatal mortality?
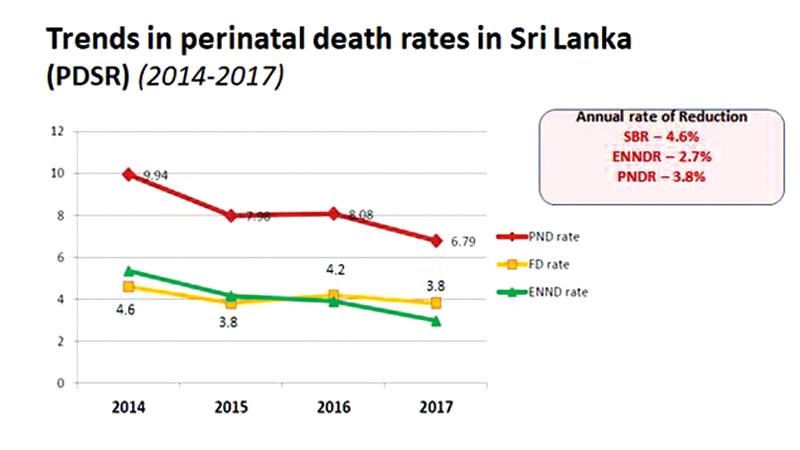
A. Basically, deaths of babies occurring in the perinatal period are perinatal deaths. The perinatal period is the duration between the 28 weeks of gestation up to 7 days after the birth of the baby.
This includes stillbirths and early neonatal deaths. Stillbirths are babies born dead in the uterus and early neonatal deaths are babies dying within seven days after birth.
Q. You were quoted as saying while addressing a press conference at the Sri Lanka Medical Association recently that 16 infants with various birth defects are born in Sri Lanka daily and that the second highest number of infant deaths was due to birth defects, with some 700 infant deaths recorded in 2018. So what is the solution to preventing perinatal deaths?
A. Counting perinatal deaths is crucial for minimising such deaths. This is called surveillance. It is the ongoing process of systematic collection, analysis, interpretation and dissemination of such data to relevant people for action. The country started perinatal death surveillance and response (PDSR) way back in 2006. We are the first country in the region to initiate PDSR and implementing it country-wide.
Q. Are there others involved in this process apart from the obstetric health providers such as neonatologists and paediatricians? Why is their participation important?
A. They are the people caring for pregnant mothers and newborns and also the data generators. They have all the information with regard to each stillbirth and neonatal death.
Q. Since Sri Lanka already had excellent health indicators regarding the reduction of maternal and infant deaths in the country, since when did perinatal deaths emerge as a priority area and a quality dimension of care in and around delivery?
A. Sri Lanka recognized perinatal deaths as a priority area in the early 2000s. The key stakeholders, paediatricians, obstetricians and community physicians got together and came up with strategies to reduce perinatal deaths. They worked together and touched on different areas of service delivery in and around delivery to achieve good birth outcomes.
In our national strategic plan on maternal and newborn health, we need a country where there are no preventable deaths of mothers, foetuses and newborns, where every pregnancy is planned and wanted, every birth celebrated, and women, babies and children survive, thrive and reach their full potential. This is our vision for all pregnancies and babies born.
Q. The Family Health Bureau (FHB ) has 12 years of experience in structured perinatal death surveillance since 2006. Tell us more about this program.
A. We started individual case reporting in 2014 and have compiled individual data covering the entire country from 2014. Each hospital with an obstetrician / paediatrician reports all the details with regard to a perinatal death that takes place in the index hospital.
Monthly compiled data are sent to Maternal and Child Morbidity and Mortality Surveillance Unit of Family Health Bureau, the country’s focal point. The coverage is very good.
For example in the year 2015, there were 1,728 still births and 1,555 early neonatal deaths when 323,735 births took place in all hospitals in the country. We process the received data annually and disseminate it to all the professionals and agencies involved in providing perinatal care for action.
Q. Of what significance is all this data? What are the benefits?
A. They are needed for National Statistics and Cross country comparisons. The Subnational / district level data with Geographic location and details on causality are essential for prevention and monitor trends. the other important aspect is for advocacy.
We can make policy makers aware of the situation with solid data. Public awareness is the other area that serves with these data.
Q. Who collects this information on newborn indicators and how?
A. A public health midwife has been assigned to each household in the country. They start from registering eligible couples and following them up. These couples are given preconception care and once a woman gets pregnant, she is taken into a register and care is provided at home, field and hospital clinics.
Once the baby is born, he is taken into another register called ‘Birth and Immunisation register’ and are followed up to five years of age.
Data is generated at each level and transferred to the central level. Some of the elements of this system are now web-based.
We have real time data. This kind of an individual level data system is not operative in any of the neighbouring countries. As such, we know what happens to each and every pregnant woman and baby in the country. Therefore, it is easy to compute maternal and newborn indicators based on solid data.
Q. I understand there was a pilot project towards setting up a data base of information on perinatal deaths. Tell us more about this project.
A. We introduced a hospital sector web-based system to collect data on perinatal deaths. This system includes all the variables recommended by WHO with regard to perinatal deaths.
The country has 105 specialised hospitals with obstetric and paediatric facilities. Family Health Bureau trained a majority of data originators from these hospitals giving a hands on exposure. Now the system is in full operation country-wide.
Q. What are the benefits 1) for mothers 2) for unborn babies?
A. With individual data collection and analysis, we identify causes, geographical locations, associated factors and most importantly service gaps related to these deaths. In addition, we conduct pathological post-mortem for a more objective determination of the cause of death. Such information is essential for the formulation of preventive strategies at individual, practice, program and policy levels.
We advise parents of the causes and the precautions they should take in future pregnancies. In caring for unborn babies, such data are important to predict complications and provide tailor-made preventive actions.
Q. What are your plans to better address the issues regarding perinatal deaths in Sri Lanka?
A. With the available data, we are planning to review these deaths in a no-fault finding modality at central level. This would be a desk review. The review panel will include experts from different specialties; paediatric, obstetric, pathology, neonatal, intensivist, etc.
The aim is to identify service gaps and translate lessons learnt into practice, programs and policies in reshaping care for the pregnant women, their unborn babies and neonates.
Q. Do you think you could realize the Millennium goal of reducing perinatal deaths by one third in 2030 ?
A. Yes. We have a target of reducing stillbirths to 2.2 per 1000 births by 2030. We have a committed healthcare force both in the field and in the hospital sector. Day by day we add quality dimensions to the care provided for pregnant women and babies. Now we are addressing on specialised care centres in strategic locations in the country.
Q. Your word of advice to mothers, family members and communities with regard to minimising fetal and infant deaths ?
A. Better planned pregnancies is number one. Continue receiving quality care obliging with advice from healthcare workers. If there is any danger feature, immediately seek care from a qualified medical officer.
Q. Your message to women on ensuring better pregnancy outcomes and reducing perinatal deaths in the country.
A. Reveal all details with regard to your health status to the healthcare workers including existing conditions such as diabetes, hypertension and heart problems. . Cooperate with the physician managing them and follow his/her advice .